Is Scoliosis Genetic? What Science Says About Family Risk
Is scoliosis genetic? Not always – but idiopathic scoliosis (the most common type) shows strong familial patterns, meaning genetics increase susceptibility without guaranteeing your child will develop curves. Growth spurts, posture, and biomechanics ultimately determine whether genetic predisposition manifests as actual scoliosis.
Understanding is scoliosis genetic helps you move past blame and focus on what actually matters: early detection, proper monitoring, and proactive treatment that can change your child’s trajectory.
Short Answer: Is Scoliosis Genetic?
Scoliosis is not always genetic, but certain types – particularly idiopathic scoliosis – often show familial patterns, meaning they tend to run in families.
Genetics increase susceptibility, not certainty. Having scoliosis in your family raises risk, but doesn’t predetermine outcomes. Growth patterns, posture, biomechanics, and early intervention significantly influence whether curves develop or worsen.
Bottom line: Family history matters, but it’s not destiny. Awareness and proactive care make the real difference.
Understanding the Main Types of Scoliosis
Not all scoliosis has the same cause or genetic component. Understanding which type your child has clarifies genetic risk.
Idiopathic Scoliosis (Most Common)
“Idiopathic” means no single identifiable cause and this accounts for 80-85% of scoliosis cases.
Characteristics:
- Strongest genetic association among scoliosis types
- Typically appears during growth years (ages 10-18)
- More common in girls than boys
- Varies widely in severity
This is the type most likely to show family patterns and genetic influence.
Congenital Scoliosis
Present at birth due to vertebrae forming abnormally during fetal development.
Developmental, not inherited. Genetics are usually not a driving factor – these structural differences occur during pregnancy, not from inherited genes.
Neuromuscular Scoliosis
Linked to neurological or muscular conditions like cerebral palsy, muscular dystrophy, or spina bifida.
Genetic influence relates to the underlying disorder, not scoliosis itself. The primary condition causes muscle imbalances that lead to spinal curvature.
Degenerative (Adult-Onset) Scoliosis
Develops from age-related spinal wear, disc degeneration, and asymmetric breakdown of spinal structures.
Not genetic, even if scoliosis existed earlier in life. This represents new curve development from mechanical breakdown, not inherited predisposition.
Is Idiopathic Scoliosis Hereditary?
Since idiopathic scoliosis shows the strongest genetic component, let’s dive deeper into familial patterns and what research reveals.
Does Scoliosis Run in Families?
Yes, statistics clearly show higher prevalence among first-degree relatives (parents, siblings, children).
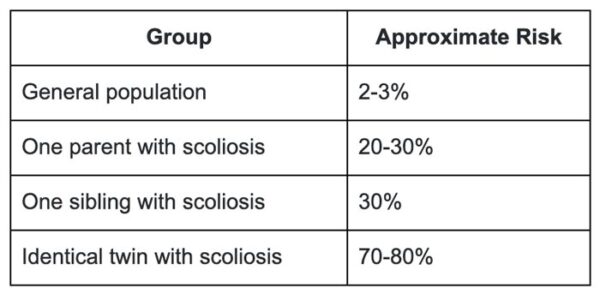
Risk increases when:
- One parent has scoliosis (20-30% higher risk for children)
- A sibling is diagnosed (approximately 30% chance for other siblings)
- Multiple family members are affected (risk compounds)
Important context: “Higher risk” doesn’t mean certainty. Most children with family history never develop significant curves.
What Genetic Research Actually Shows
There’s no single “scoliosis gene” you either have or don’t have. Instead, research reveals:
Polygenic influence: Multiple genes interacting with each other and environmental factors influence scoliosis development.
Why this matters: It explains why:
- Curves differ in severity between family members
- Some children develop curves while siblings don’t
- Timing of onset varies within families
- Progression rates differ person to person
Twin & Family Studies Explained Simply
Twin studies provide powerful genetic insights:
Identical twins (sharing 100% DNA) show higher concordance rates (both developing scoliosis) than fraternal twins (sharing 50% DNA).
What this confirms: Genetics definitely influence scoliosis risk.
What this doesn’t mean: Genetics aren’t the only factor. Even identical twins don’t always both develop scoliosis, proving environmental and biomechanical factors matter significantly.
How Much Does Genetics Increase Scoliosis Risk?
Understanding actual risk numbers helps maintain perspective without panic.
Even with strong family history, most children never develop significant scoliosis requiring treatment.
Why Risk ≠ Severity
Having genetic predisposition doesn’t predict curve severity. Two siblings might both have scoliosis, but one develops a mild 15-degree curve needing only monitoring while the other progresses to 45 degrees requiring intensive intervention.
Severity depends on:
- Growth rate and timing
- Biomechanical factors (posture, activities)
- Early detection and intervention
- Hormonal factors (especially in girls)
Why Many Genetically Predisposed Children Never Develop Curves
Genetics load the gun; environment pulls the trigger. Having genetic susceptibility creates vulnerability, but whether scoliosis actually develops depends on multiple factors beyond genetics.
Protective factors:
- Early postural awareness and correction
- Balanced physical activities
- Proper spinal biomechanics during growth
- Early screening catching subtle changes
Genetics and Curve Progression: What Really Drives Worsening?
Is scoliosis genetic in terms of progression? Partially, but biomechanics matter more.
Genetics may influence susceptibility to developing curves, but progression – curves worsening over time – is driven primarily by:
- Growth spurts: Rapid height increases create mechanical stress on already-curved spines, accelerating progression.
- Biomechanics and posture: How your child moves, sits, stands, and carries their body affects loading patterns on their spine.
- Spinal alignment: Existing postural distortions create uneven forces accelerating curve progression.
Early Detection & Screening for At-Risk Children
Catching curves early – when they’re mild and most responsive to conservative treatment – makes all the difference.
Common Screening Methods
- Visual posture analysis: Checking shoulder heights, hip levels, spinal alignment while standing normally.
- Adam’s forward bend test: Child bends forward at waist; observer looks for rib or lumbar prominence indicating rotation.
- In-clinic digital posture and spinal assessments: Advanced technology providing precise measurements tracking subtle changes over time.
- X-ray evaluation: When visual screening suggests curves, X-rays measure exact Cobb angles and spinal rotation.
What Mild Scoliosis Really Means Clinically
Mild curves (10-25 degrees) often progress unnoticed without regular monitoring – especially during growth years.
Growth years represent the most critical window. Curves that might stay stable in adults often worsen significantly in growing children.
Early = treatable: Mild curves respond beautifully to conservative correction through Chiropractic BioPhysics®, bracing, and rehabilitation. Large curves often require surgery.
Can Chiropractic BioPhysics® Help Genetically Influenced Scoliosis?
Yes – CBP® addresses the biomechanical factors determining whether genetic predisposition becomes problematic curves.
Addressing Structural Imbalance Early
CBP® targets spinal alignment and posture through:
- Mirror-image adjustments correcting curve patterns
- Specific traction protocols restoring proper spinal positioning
- Postural rehabilitation exercises
- Neuromuscular retraining
Focus on reducing abnormal loading patterns: When your spine is properly aligned, forces distribute evenly rather than concentrating on one side – slowing or stopping progression.
Studies by Morningstar et al. in Scoliosis and Spinal Disorders showed CBP® protocols significantly reduced Cobb angles in adolescent idiopathic scoliosis patients.
The Role of ScoliBrace® for High-Risk Patients
- Customized, corrective bracing using 3D scanning technology creates braces specifically designed for your child’s unique curve pattern.
- Designed for growth-phase correction: Unlike traditional braces just preventing worsening, ScoliBrace® actively works to reduce curves.
- Works alongside spinal rehabilitation strategies: Combining bracing with CBP® chiropractic care produces superior outcomes to either approach alone.
As a chiropractor Redding families trust for scoliosis management, I’ve watched the combination of CBP® and advanced bracing help countless children avoid surgery their parents feared was inevitable.
Final Takeaway: Genetics Influence Risk, Not Destiny
Is scoliosis genetic? Yes, genetics shape vulnerability – but they don’t determine outcomes.
Early awareness changes the trajectory. Knowing family history allows proactive screening, early detection, and intervention during the most treatable stages.
Non-surgical, proactive care offers meaningful control. CBP® chiropractic protocols, advanced bracing, and postural rehabilitation can significantly reduce curves and prevent progression – giving you and your child real agency over outcomes.
If scoliosis runs in your family, don’t wait for curves to develop. Schedule comprehensive screening today. Early detection during growth years provides the best opportunity for conservative correction avoiding surgery.
FAQs
Can scoliosis skip a generation?
Yes. Genetic traits don’t necessarily express in every generation. Grandparents and grandchildren might have scoliosis while parents don’t.
Why do siblings have different curve severity?
Multiple genes influence scoliosis, and each child inherits different genetic combinations. Additionally, environmental factors (growth rates, activities, posture) differ between siblings.
Is genetic scoliosis more aggressive?
Not necessarily. Curve severity and progression depend more on biomechanical factors, growth timing, and intervention than genetic vs. non-genetic origin.
Can adults pass scoliosis risk to their children?
Yes, if your scoliosis is idiopathic (not from injury or degeneration). Your children have higher risk and should receive regular screening during growth years.
